Our focused approach corrects the issue of outward-turning eyelids that can cause eye discomfort and complications. We’re committed to returning your eyelid to its natural alignment, improving your eye’s health and your overall comfort.
What is Ectropion Repair?
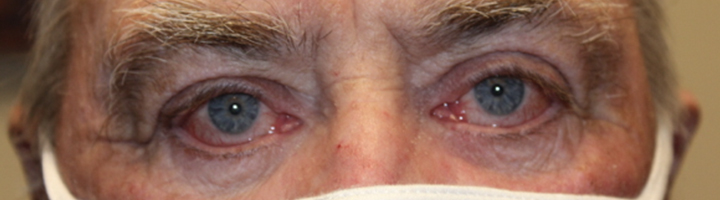
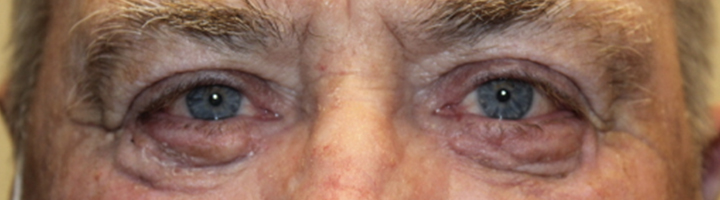
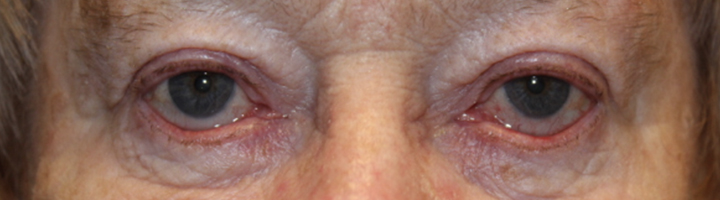
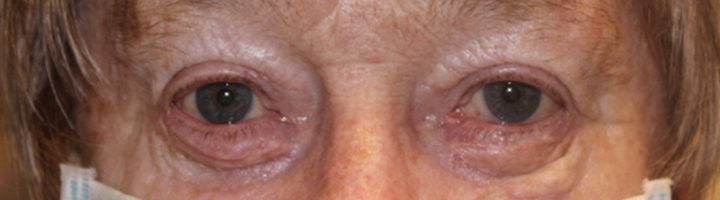
Ectropion Repair is a surgical procedure designed to correct a condition known as ectropion, where the lower eyelid turns outwards, exposing the inner surface of the eye. This condition can lead to dryness, redness, and irritation in the eye. The primary goal of Ectropion Repair is to restore the normal position of the eyelid, ensuring it properly protects and lubricates the eye.
The Procedure
Typically performed as an outpatient procedure under local anesthesia and IV sedation, Ectropion Repair involves a small incision near the inside of the lower lid or below the lash line area. In more severe cases additional skin may be added to the lower lid to help with the repositioning while in more straight foreword cases tightening the lower lid at the outer corner is the utilized approach.
Benefits
Ectropion Repair can dramatically improve eye comfort, reduce dryness and redness, and prevent potential corneal damage caused by excessive exposure.
Alternatives
For those unable to have surgery, temporary measures such as artificial tears or lubricating ointments can help mitigate symptoms. However, these alternatives do not address the root cause and surgical treatment is usually recommended for a long-term solution.
We urge patients to discuss any concerns with their surgeon, to ensure peace of mind prior to proceeding with surgery.
Ectropion Repair Before & After
Medical Disclaimer: The photos below are of patients who received care at Northwest Eyelid & Orbital Specialists. Please note that individual outcomes of any surgical procedure can vary greatly. The before and after images shown here represent results achieved for specific patients – they should not be interpreted as a guarantee or implication of similar results for all patients.
Each individual’s treatment and/or results may differ due to a variety of factors including overall health, lifestyle, and other unique circumstances.
We work diligently to achieve the best possible outcomes for all our patients without guaranteeing identical results for every patient.
I highly recommend Dr Michels ! He was very kind and took his time explaining the procedure I was going to have. The whole experience was excellent. The staff we so helpful ,professional and thorough with every step. My outcome was more than I hoped for since it was a skin cancer procedure on my eyelid. He genuinely cares about his patients and providing the best care possible
-D
★★★★★5/5
Due to my droopy eyelids & impaired vision, Dr. Kevin Michels performed successful eyelid ptosis surgery on me in December 2022. Dr. Michels and his staff were very courteous and professional, and I would highly recommend Northwest Eyelid & Orbital Specialists.
-T
★★★★★5/5
Dr. Michels and his staff have been amazing!! If I could give them 10 stars I would. I was treated with kindness and respect. I would describe Dr. Michels ability as surgical artistry. Having the weight off my eyelids after Bells Palsy is a dream come true. Thank you Dr. Michels & Team!!!
-S
★★★★★5/5
I highly recommend Dr Michels ! He was very kind and took his time explaining the procedure I was going to have. The whole experience was excellent. The staff we so helpful ,professional and thorough with every step. My outcome was more than I hoped for since it was a skin cancer procedure on my eyelid. He genuinely cares about his patients and providing the best care possible
-D
★★★★★5/5
Due to my droopy eyelids & impaired vision, Dr. Kevin Michels performed successful eyelid ptosis surgery on me in December 2022. Dr. Michels and his staff were very courteous and professional, and I would highly recommend Northwest Eyelid & Orbital Specialists.
-T
★★★★★5/5
Dr. Michels and his staff have been amazing!! If I could give them 10 stars I would. I was treated with kindness and respect. I would describe Dr. Michels ability as surgical artistry. Having the weight off my eyelids after Bells Palsy is a dream come true. Thank you Dr. Michels & Team!!!